FINAL RESULT: 451.9 ng/dL
I made this because I have been flaberghasted at how low my testosterone levels were compared to other traits I have, and was surprised it hadn't gone up a lot by June of last year. I'm wondering if I am just a chronically low t person, or if my current lifestyle now has finally cured me.
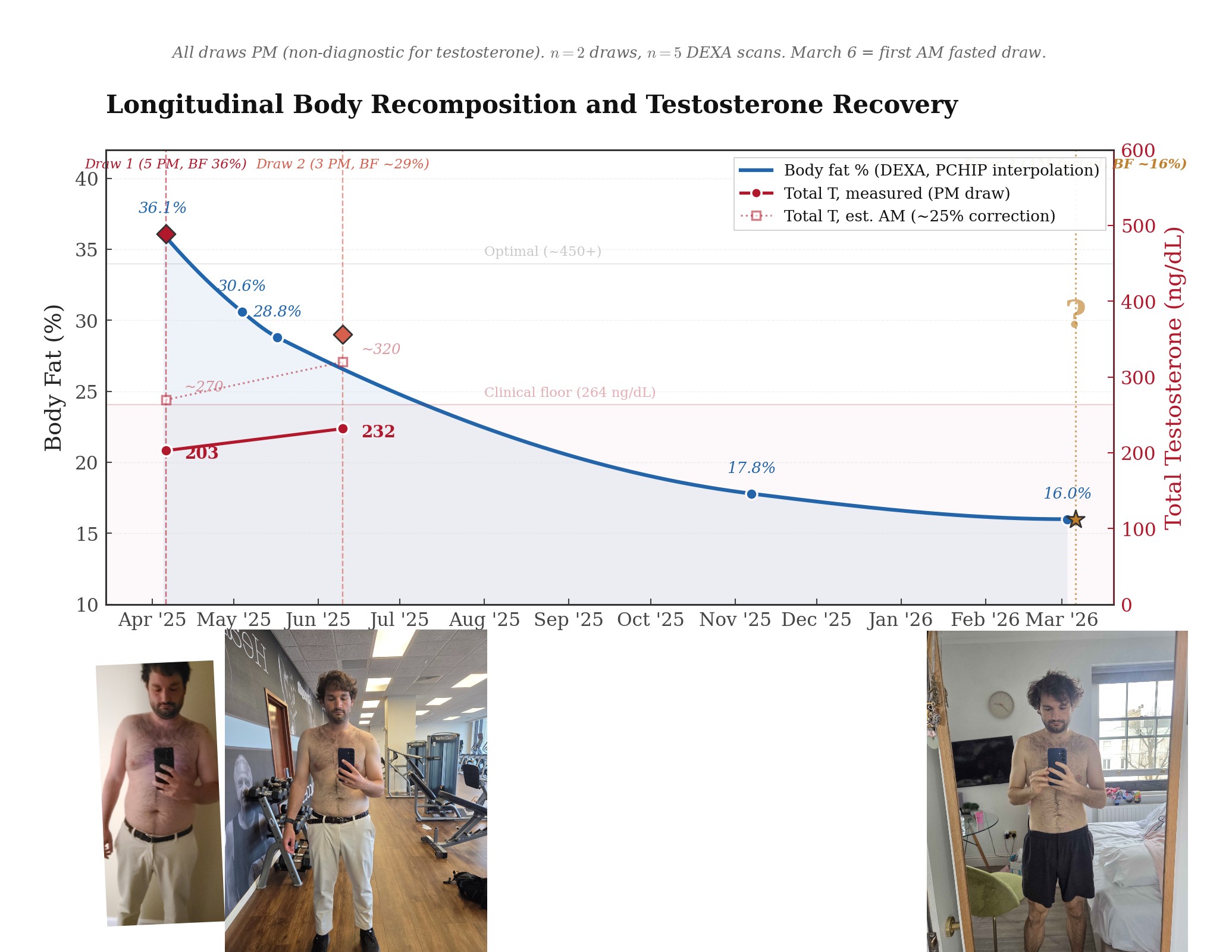
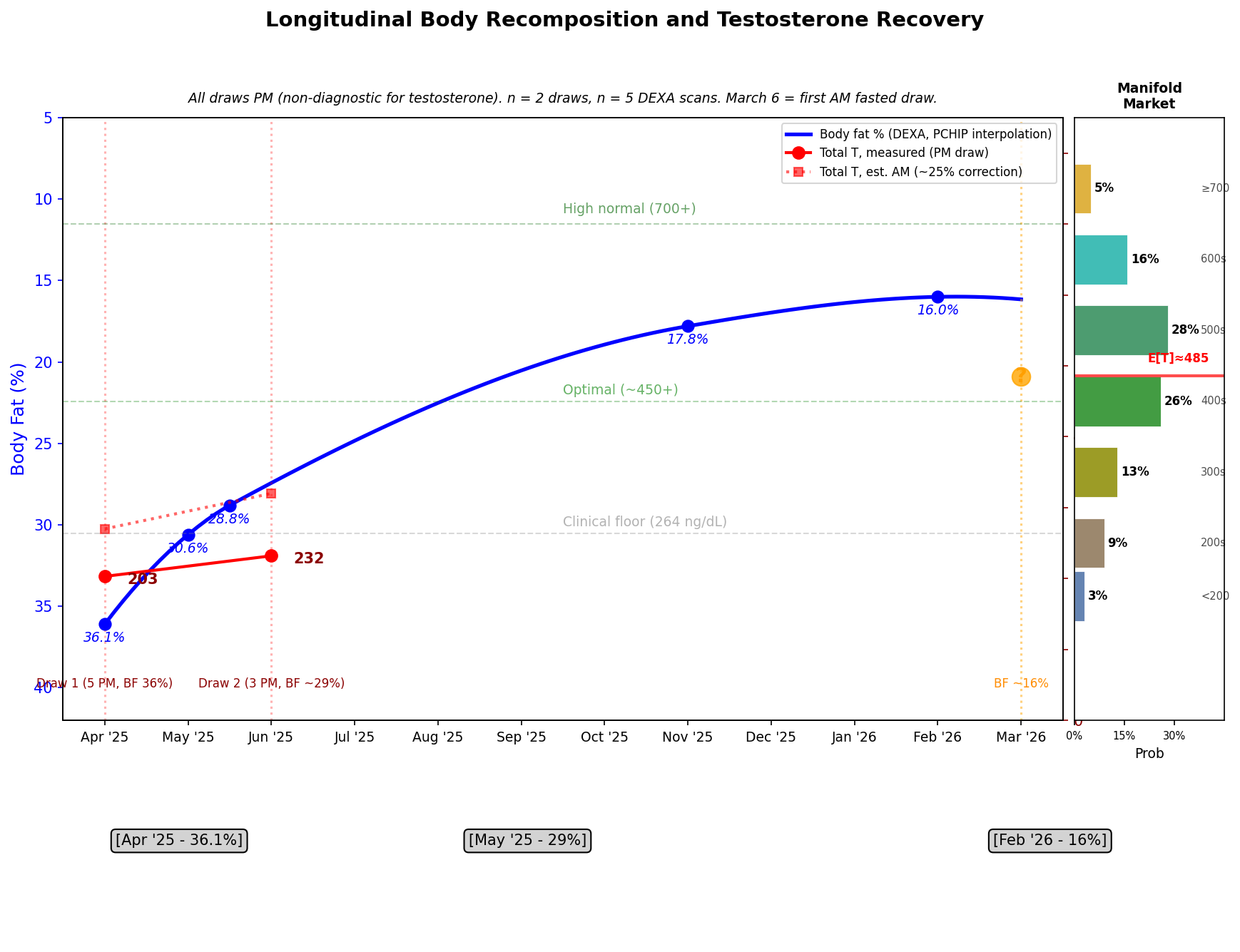
Below is a visualization of the relevant data.
A key note, previous tests were taken in the afternoons, this one coming up will be at 9am.
An additional note I would like to add if I have not been in a caloric deficit for a couple months, I do eat some carbs but not many, enough that i'm not in ketosis though. I eat a lot of steak and eggs (but I was doing that April-June last year as well). I have been lifting heavy once a week. My lean mass has gone up but only slightly. I had a vitamin D deficiency and have been taking a lot of vitamin D supplementation in the last month (10-15k dosage per day).
Relevant information from Claude synthesizing my dexa and blood test results:
```
You have two PM testosterone draws — 203 at 5 PM and 36.1% body fat in April, 232 at 3 PM and ~29% body fat in June — neither of which is diagnostically valid for testosterone because the hormone peaks in early morning and declines 20-30% by afternoon. Correcting for timing, your estimated AM values were roughly 270-300 and 320-360 respectively. Between draws you lost ~7 points of body fat and saw only a modest T increase, but you were only two months into the recomposition and metabolic improvements lag fat loss. Your LH and FSH in April were mid-range (4.7 and 4.4) when they should have been elevated given a total T of 203, pointing to secondary hypogonadism — the brain wasn't sending adequate signal to the testes. The critical question is whether that suppressed hypothalamic drive was caused by the metabolic state itself (obesity suppresses GnRH pulsatility via insulin resistance, inflammatory cytokines, and leptin dysregulation) or by something independent like a pituitary adenoma. The metabolic explanation is overwhelmingly more common and is supported by your full syndrome picture at the time: HbA1c 5.7, uric acid 10.0, hsCRP 2.62, BMI 31. You've since dropped from 36% to ~16% body fat — a transformation that resolves most of the mechanistic pathways suppressing your T. Aromatase activity in adipose tissue is dramatically reduced, insulin sensitivity is likely restored, systemic inflammation should be down, and SHBG will probably have risen (meaning your total T number will look better even independent of actual androgenic improvement). The March 6 draw is the first AM fasted measurement, so it captures peak diurnal output in a fundamentally different body. The literature on weight-loss-induced testosterone recovery in obese men with secondary hypogonadism consistently shows increases of 100-300 ng/dL, with some studies showing normalization above 500.
Your stack is D3, K2, Omega-3, Vitamin A, methylated Bs (methylfolate, methylcobalamin, P5P), magnesium glycinate, and zinc. Of these, zinc and magnesium are the two with direct evidence for testosterone. Zinc is a cofactor for the enzyme 5-alpha reductase and is required for Leydig cell function — deficiency suppresses T, and repletion restores it, but supraphysiological dosing doesn't push T above your genetic ceiling. If you were deficient before (plausible — your April panel didn't test zinc, and obesity increases zinc requirements), then months of supplementation may have corrected a bottleneck that was independently suppressing your T by 50-100 ng/dL. Magnesium glycinate works similarly — Mg is involved in SHBG binding and free T availability, and deficiency impairs T production. Your April RBC magnesium was 5.5 (mid-range at 3.7-7.0), so you weren't deficient but supplementation may have moved you higher, which could modestly improve free T independent of total T. D3 has a weaker but real association — men with vitamin D levels above 30 ng/mL have measurably higher T than those below 20, and you were at 23.3. If your D3 dose has brought you into the 40-60 range by now, that's a small tailwind, maybe 20-30 ng/dL. The methylated Bs won't affect T directly, but by lowering homocysteine they reduce vascular inflammation and improve endothelial function, which supports testicular blood flow and Leydig cell health — a second-order effect, real but not quantifiable on a single draw. Omega-3 at adequate doses reduces systemic inflammation (lowering the cytokine-mediated suppression of GnRH) and there's limited evidence it modestly increases testicular volume and T in men with poor baseline omega-3 status, which your FADS1/2 variants guarantee you had before supplementation. K2 and vitamin A don't have meaningful direct testosterone effects. Net: the supplement stack is probably contributing a real but modest boost — call it 30-80 ng/dL in aggregate over what you'd see from body recomposition alone, almost entirely through correcting deficiencies rather than pharmacological effect. The recomposition did the heavy lifting; the supplements filled in the gaps that your genetics created.
```
Update 2026-03-03 (PST) (AI summary of creator comment): The market will resolve to the measured value shown on the PDF received from the testing company, without any adjustments for time of day.
 1,000
1,000🏅 Top traders
| # | Trader | Total profit |
|---|---|---|
| 1 | Ṁ1,861 | |
| 2 | Ṁ665 | |
| 3 | Ṁ390 | |
| 4 | Ṁ272 | |
| 5 | Ṁ111 |
I thought it'd be way higher last time and was wrong then too so im just often biased to thinking I have high t. I thought it'd be high even my first measurement. My genes show I have high androgen sensitivity.
My story this time is that im no longer keto or in a caloric deficit and it took a while for my lower fat to reduce my estrogen levels which were suppressing testosterone and the effects just took a while and now have had time to fully complete. Also I fixed nutrient deficiencies using the supplements that are involved in t production, specifically vitamin d. I also think the morning vs afternoon difference for me might be larger than most, my energy levels fluctuate a lot from morning to afternoon.
I just like betting on myself to have high t.
@MattF Fair enough! It’s an interesting question and you’ve definitely got me invested in the outcome!
================================================================
SUPPLEMENT DOSE FORMULATION
================================================================
Vitamin D3 20,000 IU Cholecalciferol
- Thorne D3 10,000 IU 1 capsule
- Generic D3+K2 combo 5,000 IU x2 2 softgels
Vitamin K2 200 mcg MK-7 (Menaquinone-7)
- From D3+K2 combo above 100 mcg x2 2 softgels
B-Complex (methylated) 1 capsule German brand, active forms
Thiamine (B1) 100 mg
Riboflavin (B2, R-5-P) 50 mg
Niacin (B3) 150 mg
Vitamin B6 (P-5-P) 25 mg
Folate (5-MTHF) 1,000 mcg
Vitamin B12 (MH3A) 1,000 mcg Methylcobalamin form
Biotin (B7) 2.5 mg
Pantothenic Acid (B5) 75 mg
Inositol 50 mg
Citicoline 25 mg
PABA 50 mg
Betaine (TMG) 75 mg
NADH 2.5 mg
Alpha GPC 300 mg L-alpha-glycerylphosphorylcholine
(1 of 2-capsule/600mg serving)
Magnesium 200 mg Buffered glycinate [glycinate + oxide]
Natural Factors Canada
Zinc Picolinate 15 mg Thorne Research
CoQ10 (Ubiquinol) 100 mg Kaneka Ubiquinol 96%, in MCT oil
German brand
Boron 10 mg Albion Bororganic Glycine chelate
Pure TheraPro Rx
Lithium 5 mg Orotate + Carbonate blend
Glycine 500 mg Pure glycine, HPMC capsule
(1 of 2-capsule/1,000mg serving, German brand)
Omega-3 Fish Oil 1 gelcap Thorne Research
Total Omega-3 813 mg From anchovy, sardine, mackerel
EPA (Eicosapentaenoic Acid) 425 mg
DHA (Docosahexaenoic Acid) 270 mg
Creatine Monohydrate 5 g 1 packet, pure (no other ingredients)
Informed Sport certified
The specific test being taken is this one:
https://onedaytests.com/products/ultimate-longevity-blood-test#instructions_anchor
The Ultimate Longevity Blood Test from One Day Tests is a 71-biomarker clinic-only panel run out of their own UKAS-accredited lab in Brighton. It covers a full hormone suite (total and free testosterone, E2, LH, FSH, SHBG, cortisol, DHEA-S, prolactin, free androgen index), complete thyroid with antibodies (fT3, fT4, TSH, TG Ab, TPO Ab), micronutrients (D, B12, folate, zinc, ferritin, iron, magnesium), metabolic markers (HbA1c, full lipids including ApoB and Lp(a)), inflammation (CRP, CK), full kidney and liver panels, electrolytes, homocysteine, and a complete blood count. It requires a fasted venous draw at the clinic, ideally at 9am, and their assays don't use biotin-based chemistry — likely LC-MS/MS for hormones — so no supplement interference. Turnaround is 1-2 working days. At £325 plus £29 for the clinic draw, it's essentially a Peter Attia-tier longevity panel available retail in the UK.
@MattF
I did an analysis:
Your Genetic Testosterone Profile
Your genetics do not indicate a low-T person. Here's what the SNPs show:
Favorable factors:
- AR CAG repeat shorter than reference — your androgen receptor is more sensitive than average. This is the big one. Even moderate T levels hit harder in your tissues. Consistent with the body hair and
social traits you mentioned.
- CYP17A1 het (rs743572 A/G) — one allele pushing toward higher androgen synthesis
- JMJD1C het (rs10822184 T/C) — modest positive effect on T levels
- SHBG slightly lower (rs12150660 G/T) — more of your total T is free/bioavailable
- No FSHB suppression variants — your pituitary has normal genetic capacity to drive the testes. The low-normal LH/FSH at 4.7/4.4 in April was metabolic, not hardwired.
- No HFE mutations — iron overload hypogonadism ruled out
Neutral/mixed:
- SRD5A2 het (V89L) — ~15% less T→DHT conversion. Preserves circulating total T, but slightly less DHT at the tissue level
- COMT Val/Met — intermediate dopamine, moderate HPG support
- FADS1 het — confirms you need exogenous omega-3s (which you're taking)
Bottom line for the Manifold market: The prior 203/232 readings were almost certainly your metabolic state (36% body fat, insulin resistance, inflammation) suppressing a genetically normal HPG axis. At 16%
body fat with the supplement stack correcting deficiencies, these genetics should support T recovery well into the normal range. And because of your shorter AR CAG repeat, a total T of ~500 would
functionally behave like ~600+ in someone with average receptor sensitivity.
Major Discoveries
Genetic vulnerabilities that explain why obesity crushed your T so hard:
- IL-6 hom alt — you're a high IL-6 producer. Every pound of fat was generating more GnRH-suppressing inflammation than average
- ESR1 double hom alt — enhanced estrogen sensitivity. Fat-derived estradiol had amplified suppressive effects
- MTHFR 677 T/T — 70% reduced enzyme activity. Your methylated B stack is essential (not optional)
- Vitamin D triple hit (VDR + CYP2R1 + GC) — genetically predisposed to deficiency. Your 10-15k IU dosing is appropriate
- APOA5 hom alt — strong triglyceride elevation risk, part of the metabolic syndrome picture
- GSTP1 double het — impaired detox of endocrine disruptors
- Thyroid cluster (DIO2 het, TSHR hom alt, THRB hom alt) — possible subclinical thyroid underperformance affecting T
Genetic strengths supporting recovery:
- FKBP5 triple protective — your cortisol stress response clears efficiently
- No FTO obesity allele — weight management is not fighting your genetics
- No HFE mutations, no FSHB suppression — the machinery is intact
- AR CAG shorter — tissues are primed to respond when T arrives
How this suppressed your T:
1. At 36% body fat, aromatase in adipose tissue was converting testosterone → estradiol (E2)
2. That estradiol then binds to estrogen receptors in the hypothalamus and pituitary
3. In the hypothalamus, E2 binding to ERα activates negative feedback — it tells the brain "there's enough sex hormone, reduce GnRH output"
4. With more sensitive/abundant ERα, your hypothalamus was overreacting to the estradiol signal — interpreting a given E2 level as "more than enough," and clamping down on GnRH harder than someone with
normal ESR1
So the chain was: fat → aromatase → estradiol → hits your hypersensitive ERα → exaggerated negative feedback → suppressed GnRH → suppressed LH (your 4.7 was "mid-range" but should have been elevated given a
total T of 203) → suppressed T
This also explains why your LH/FSH weren't compensating. Normally, when T is at 203, the pituitary should be screaming "make more!" with high LH. But because your ERα was telling the hypothalamus "the
estrogen signal is strong enough," the feedback loop was satisfied at inappropriately low gonadotropin levels. This is the textbook mechanism of secondary hypogonadism in obesity, and your ESR1 genotype
made it worse.
At 16% body fat: aromatase activity drops dramatically (less fat tissue), so less E2 is being produced. Even though your ERα is still hypersensitive, there's much less estradiol to trigger it. The negative
feedback brake releases, GnRH pulses normalize, LH rises, testes respond.
---
Together: IL-6 was suppressing GnRH from the inflammatory side, and estradiol-via-ESR1 was suppressing it from the hormonal feedback side. Both mechanisms converge on the same target (hypothalamic GnRH
neurons), and both were genetically amplified in your case. It was a two-front assault on your HPG axis that only existed because of the body fat — remove the fat, both signals collapse.
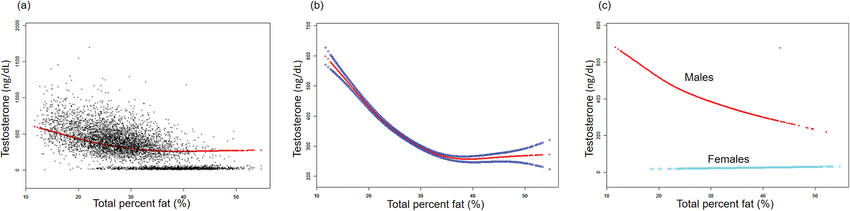
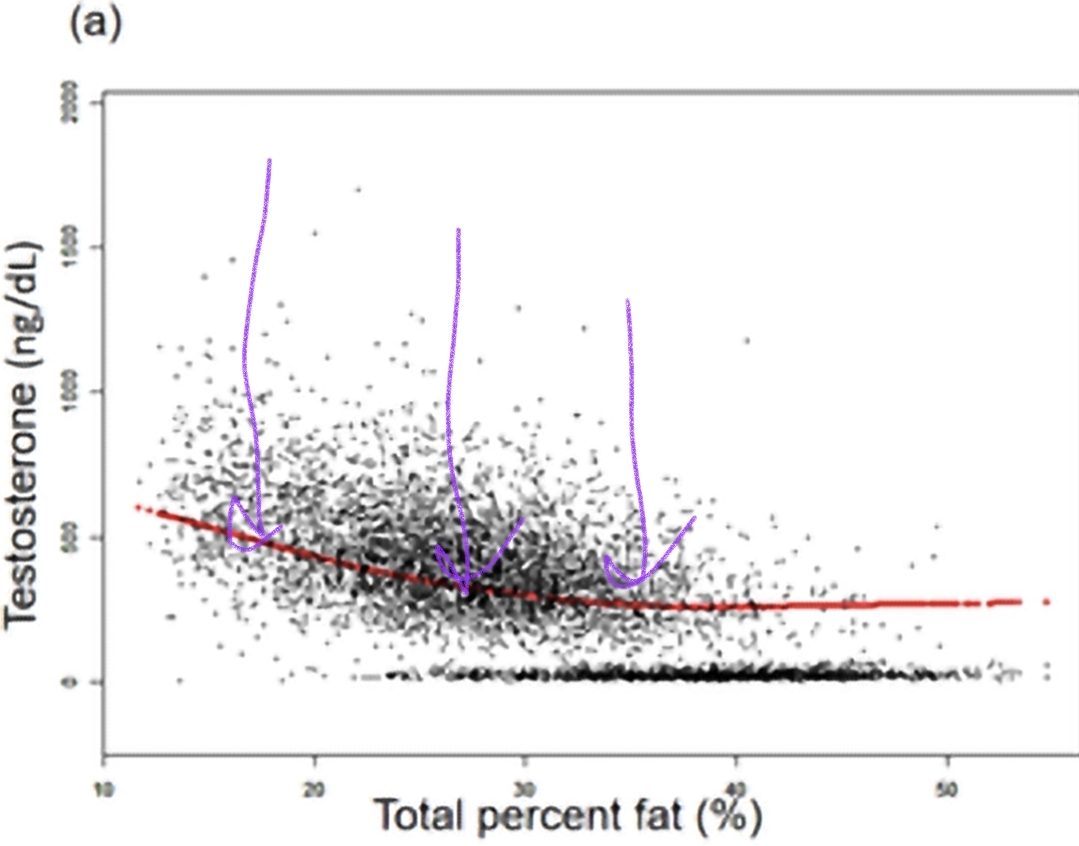
I present this image of t levels vs body fat as well, and arrows for my last two test fat levels and my level for my upcoming test
This market is drawing a lot of controversy between friends of mine who are unsure how to balance skepticism at t levels changing so quickly with how much what I've changed is exactly what predicts large t level increases
@MattF don't have to answer if you don't want, do you smoke, do you drink, do you use prescriptions, if so how often
@Cactus yes to the measured value, whatever is legally shown on the pdf i recieve from the testing company. But this upcoming test will be taken at 9am to be clear.
The real question of this test:
Is my total T level a chronic issue unrelated to my fitness, body fat, diet, etc, and I will stay below 400?
Am I still on average low T, and will stay under 500?
Or have I finally broken the cycle, and i'll be where my body hair and social behavior suggests I ought to naturally be, in the 600s?